Joint replacement surgery is a common and highly effective procedure for relieving pain, improving mobility, and enhancing the quality of life for individuals with severe joint damage. Whether due to arthritis, injury, or other conditions, when conservative treatments like medication and physical therapy no longer provide relief, joint replacement may be the next step. Whether you’re considering this surgery for yourself or a loved one, understanding what to expect before, during, and after the procedure can help you make informed decisions and prepare for a successful recovery.
What is Joint Replacement Surgery?
Joint replacement surgery involves removing the damaged or diseased parts of a joint and replacing them with artificial components, called prostheses. These prostheses are typically made of metal, plastic, or ceramic materials designed to mimic the natural movement of a healthy joint. The goal of the surgery is to relieve pain and restore function to the joint, allowing patients to return to their normal activities with improved mobility and less discomfort.
The most common types of joint replacement surgeries include:
1. Knee Replacement – Replace the knee joint with an artificial knee, commonly used for osteoarthritis or other knee conditions.
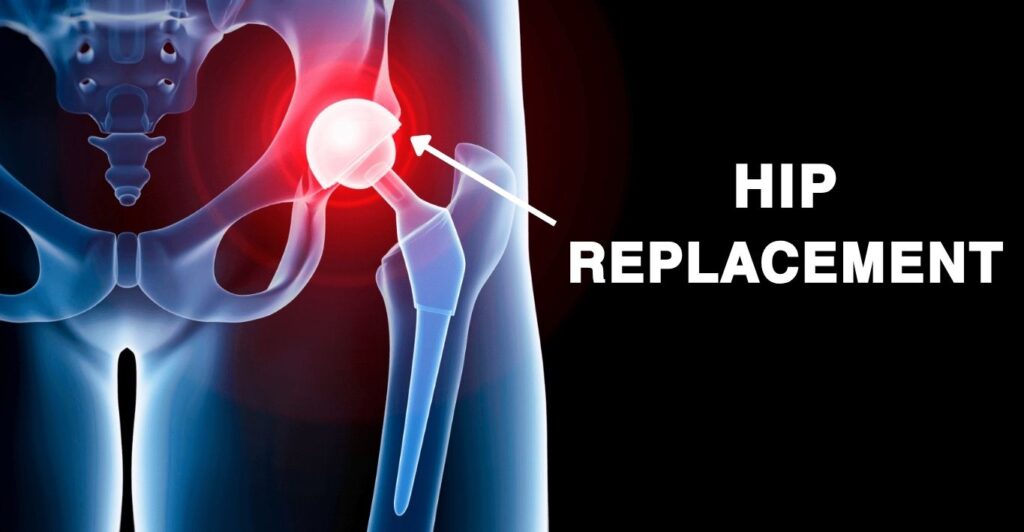
2. Hip Replacement – Replace the hip joint with an artificial hip, often used to treat arthritis or severe fractures.
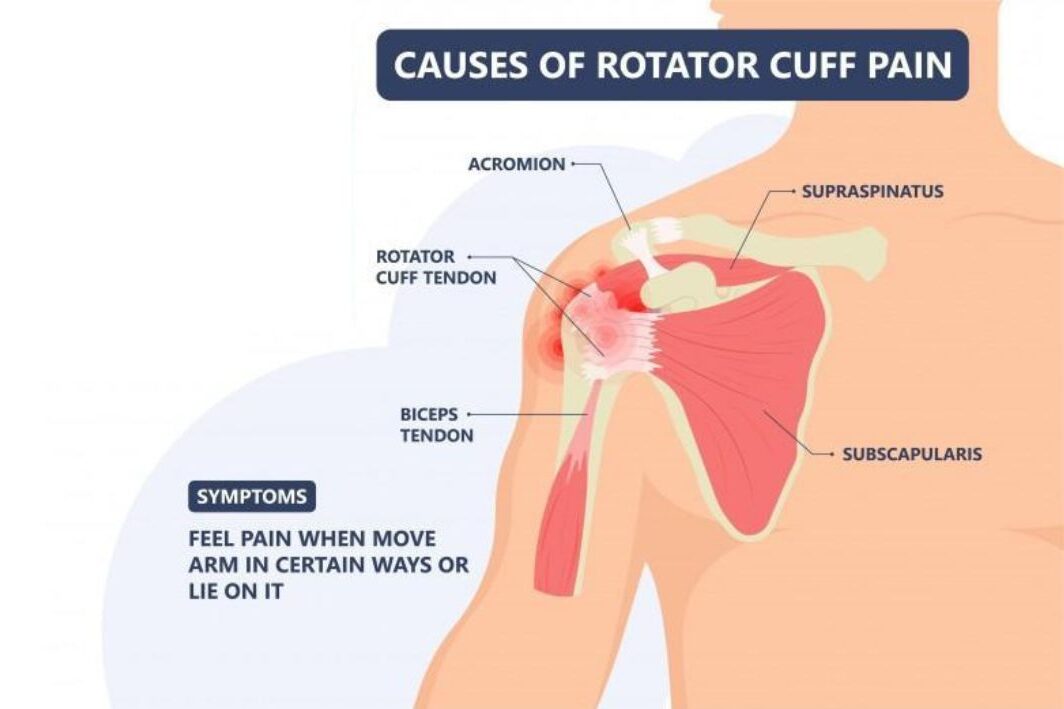
3. Shoulder Replacement – Replace the shoulder joint with an artificial shoulder, typically for severe arthritis or rotator cuff injuries.
4. Ankle Replacement – Replace the Ankle joint with an artificial Ankle, commonly used for total ankle arthroplasty.
Each type of joint replacement is tailored to address specific conditions, such as osteoarthritis, rheumatoid arthritis, post-traumatic arthritis, or other degenerative joint diseases.

When is Joint Replacement Surgery Recommended?
Joint replacement surgery is typically recommended for individuals with severe joint damage that significantly impacts their quality of life. Joint replacement surgery is considered when joint pain and dysfunction severely impact a person and other treatment options have been exhausted.
The most common conditions that lead to joint replacement include:
1. Osteoarthritis – The most common reason for joint replacement, osteoarthritis is a degenerative joint disease that causes the breakdown of cartilage, leading to pain, stiffness, and swelling.
2. Rheumatoid Arthritis – This autoimmune disorder causes inflammation in the joints, leading to pain and deformity. Over time, it can severely damage the joint, making replacement necessary.
3. Post-Traumatic Arthritis – This type of arthritis develops after an injury to the joint, such as a fracture or dislocation, which can lead to long-term damage and degeneration.
4. Avascular Necrosis – A condition where the blood supply to the bone is disrupted, leading to bone death and joint collapse, often necessitating joint replacement.
5. Severe Joint Injuries – In some cases, severe fractures or joint injuries that cannot be repaired with other treatments may require joint replacement.
Joint replacement is usually considered when:
1. Chronic Joint Pain – Pain persists despite non-surgical treatments like physical therapy, medications, or lifestyle changes.
2. Limited Mobility – Difficulty performing daily activities, such as walking, climbing stairs, or getting in and out of chairs, due to joint stiffness and pain.
3. Reduced Quality of Life – The joint pain and mobility limitations significantly impact your ability to enjoy life, affecting your mental and emotional well-being.
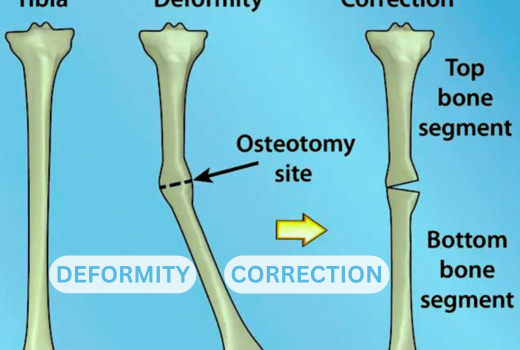
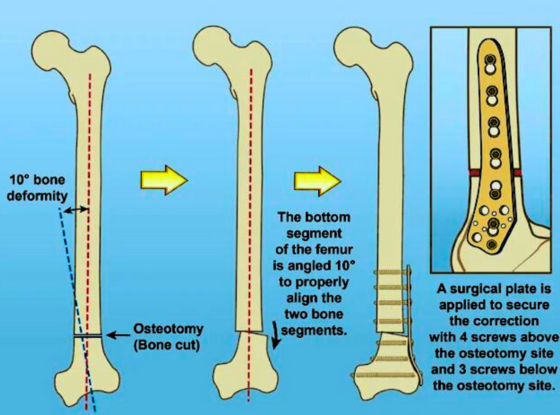
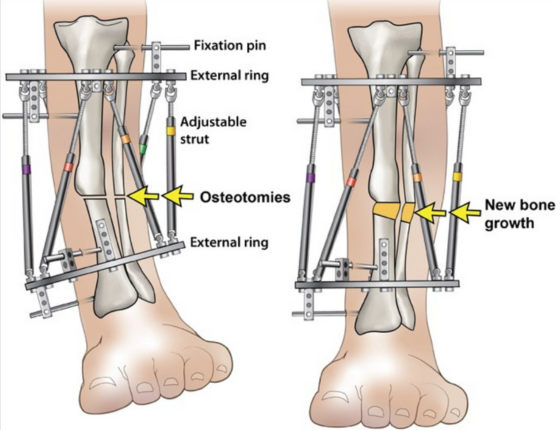
4. Joint Deformity – Noticeable deformity of the joint, often due to advanced arthritis, which cannot be corrected by other means.
5. Severe Pain – Persistent pain that limits daily activities and isn’t relieved by non-surgical treatments such as medications, physical therapy, or injections.
6. Loss of Function – Significant loss of joint function that affects the ability to perform routine activities like walking, climbing stairs, or grasping objects.
7. Advanced Joint Damage – Extensive damage to the joint due to conditions such as osteoarthritis, rheumatoid arthritis, or traumatic injury.
Your orthopedic surgeon will evaluate your condition through a combination of physical examinations, imaging tests (like X-rays or MRIs), and a review of your medical history before recommending surgery.
Recovery and Rehabilitation:
Recovery from joint replacement surgery is a gradual process that involves:
1. Physical Therapy – Physical therapy is essential to restore movement and strength in the new joint. You’ll likely start with simple exercises in the hospital and continue with outpatient therapy after discharge.
2. Pain Management – Pain and swelling are normal after surgery, but they can be managed with prescribed medications and ice packs.
3. Mobility Aids – You may need to use crutches, a walker, or a cane for several weeks to months after surgery to assist with walking.
4. Follow-Up Appointments – Regular follow-up visits with your surgeon will monitor your progress and address any concerns. These appointments are crucial to ensuring proper healing and the long-term success of the joint replacement.
5. Returning to Activities – While most people can return to normal activities within a few months, it’s important to avoid high-impact activities that could damage the new joint. Low-impact exercises, like swimming, cycling, and walking, are encouraged.
For more information talk to a healthcare provider.
If you have any questions about Joint Replacement Surgery, please feel free and leave a comment.
Do share this blog with your friends and family!